 Kate Gillie
Kate Gillie
POTUS
Yesterday kicked Mental Health (MH) Advocacy back a century. In one quick press conference he itemized a system of reporting and cataloguing any individual seeking help with MH challenges whilst in the same breath stating he was working towards eliminating MH STIGMA.
I’ve always thought the best way of defeating the STIGMA around a particular challenge or identity to be to establish a list that will be used against an individual admitting to being of that ethnicity/human grouping. Walk into a counselor’s office in the US after yesterday’s POTUS announcement and ask for help with your PTSD, you run the risk of being slapped onto the the President’s list. Worked for the Nazi’s in WWII, why not for the President of America?
What a wanker.
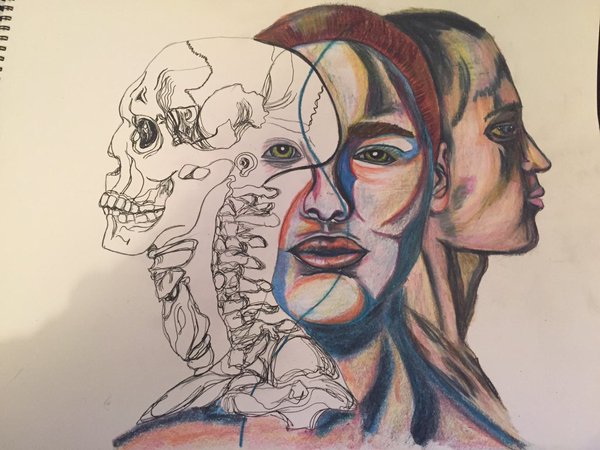
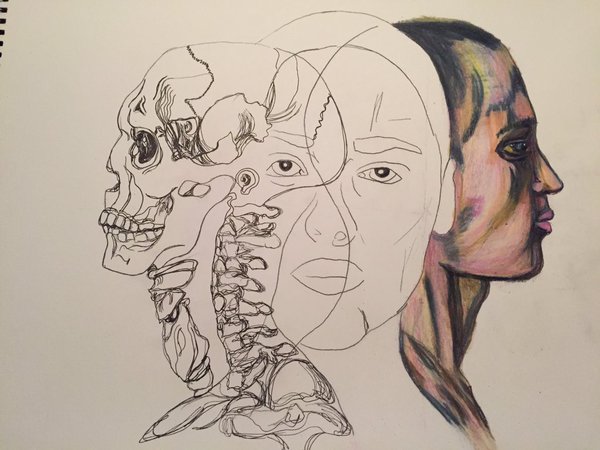
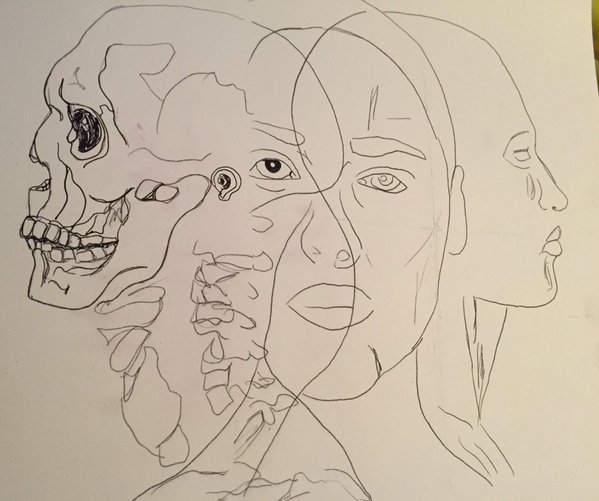
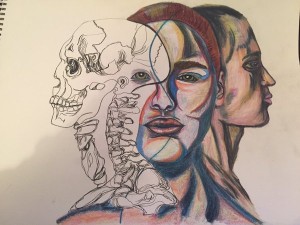
What is it like to live with #PTSD Mr President? Take a look at that art piece I did and read:
MIND
– Flashbacks – a re-run of the event(s) ‘flashes’ before our eyes, it was sometimes hard for me to know which was reality, the flashback or the present. The one is so loud and clear. The other dulled. It’s one of the first skills we learn when fixing our injury is to remain ‘present’ – by taking notice of our surroundings, counting tiles, describing the decor in our heads or out loud… anything to not go back to the hell that hurt us.
– Depression – when in danger we are wired to remain in the cave, quiet and isolated until the danger has passed. That’s one of the reasons the brain pushes us to depression when we are triggered; when we are in a situation that reminds us of the time we were injured.
– Fears and phobias – places/smells/sounds/tastes/sights/touching objects that remind us of … the world is so full of innumerable cues to send us back to hell.
– Nightmares – left me physically bruised. Still, on occassion, I will wake up beaten. When it’s bad I wake up feeling like I spent the night on a spin cycle in a cement mixer.
– Interpersonal problems – trust, anxiety, sensitivity, anger/fear… you name it, we live with it. Move forward from it. Injured but not a life sentence, we take our recovery and we push to be free of the thing(s) that hurt us. It requires a village to bring up a chid; it requires a village to get us back to health.
SOUL
Loss of purpose/pleasure – how to see the beauty of life or the possibilities of the future when all there is is pain?
Existential crisis – what’s the point of it all? Why keep going? Loss of hope, loss of self, loss of the very fabric and foundations of our existence. How to find our way through on the constant chaos of negative thought, the disturbing and destructive thoughts that remind us of what happened.
Proxy Self – offering the world and ourselves a made up version of ourselves; developed to protect us, it enivitably traps and retards our ability to heal.
No Self-Worth – self explanatory, this is key to recovery. Our self-worth has to start with SELF, not in others. But we must chose to find ourselves worthy of happiness, joy, kindness and empathy. Too often we fall into the trap of being ‘protected’ and ‘saved’ by others – this simply keeps us feeling a victim, of little worth and permanently trapped in PTSD.
BODY
Panic Attacks – about as fun as stabbing yourself in the eye with a pencil. Humiliating and vile.
Self-harm – a way of releazing endorphins to no longer feel, see, hear… what happened.
Sleep/Eating Problems – how to sleep when you know the nightmares are waiting? And eating? Why would I feed me when I can’t see the point of any of it.
Gynaecological Problems and Sexual Dysfunction – obvious, but too little focus given to this. It is made worse by the monster drugs we are regularly slammed on.
Headaches/Migraines – a constant and unremitting torture.
High Blood Pressure – for some, others of us simply flat line.
So, there you have it.
That is what living with PTSD is. President of the United States answer to this is to slap us on a registration list? Because after serving their country, their state, the people of the US or surviving an abusive childhood/marriage that’s the best thing to do?
Wanker.